Biomedical Imaging by Youxin Mao - HTML preview
Download the book in PDF, ePub, Kindle for a complete version.
I
Biomedical Imaging
Biomedical Imaging
Edited by
Youxin Mao
In-Tech
intechweb.org
Published by In-Teh
In-Teh
Olajnica 19/2, 32000 Vukovar, Croatia
Abstracting and non-profit use of the material is permitted with credit to the source. Statements and
opinions expressed in the chapters are these of the individual contributors and not necessarily those of
the editors or publisher. No responsibility is accepted for the accuracy of information contained in the
published articles. Publisher assumes no responsibility liability for any damage or injury to persons or
property arising out of the use of any materials, instructions, methods or ideas contained inside. After
this work has been published by the In-Teh, authors have the right to republish it, in whole or part, in any
publication of which they are an author or editor, and the make other personal use of the work.
© 2010 In-teh
www.intechweb.org
Additional copies can be obtained from:
publication@intechweb.org
First published March 2010
Printed in India
Technical Editor: Melita Horvat
Cover designed by Dino Smrekar
Biomedical Imaging,
Edited by Youxin Mao
p. cm.
ISBN 978-953-307-071-1
V
Preface
Biomedical imaging is becoming an indispensable branch within bioengineering. This research
field has recent expanded due to the requirement of high-level medical diagnostics and rapid
development of interdisciplinary modern technologies. This book is designed to present the
most recent advances in instrumentation, methods, and image processing as well as clinical
applications in important areas of biomedical imaging. This book provides broad coverage of
the field of biomedical imaging, with particular attention to an engineering viewpoint.
Chapter one introduces a 3D volumetric image registration technique. The foundations of
the volumetric image visualization, classification and registration are discussed in detail.
Although this highly accurate registration technique is established from three phantom
experiments (CT, MRI and PET/CT), it applies to all imaging modalities. Optical imaging has
recently experienced explosive growth due to the high resolution, noninvasive or minimally
invasive nature and cost-effectiveness of optical coherence modalities in medical diagnostics
and therapy. Chapter two demonstrates a fiber catheter-based complex swept-source optical
coherence tomography system. Swept-source, quadrature interferometer, and fiber probes
used in optical coherence tomography system are described in details. The results indicate that
optical coherence tomography is a potential imaging tool for in vivo and real-time diagnosis,
visualization and treatment monitoring in clinic environments. Brain computer interfaces have
attracted great interest in the last decade. Chapter three introduces brain imaging and machine
learning for brain computer interface. Non-invasive approaches for brain computer interface
are the main focus. Several techniques have been proposed to measure relevant features from
EEG or MRI signals and to decode the brain targets from those features. Such techniques
are reviewed in the chapter with a focus on a specific approach. The basic idea is to make
the comparison between a BCI system and the use of brain imaging in medical applications.
Texture analysis methods are useful for discriminating and studying both distinct and subtle
textures in multi-modality medical images. In chapter four, texture analysis is presented as
a useful computational method for discriminating between pathologically different regions
on medical images. This is particularly important given that biomedical image data with near
isotropic resolution is becoming more common in clinical environments.
VI
The goal of this book is to provide a wide-ranging forum in the biomedical imaging field
that integrates interdisciplinary research and development of interest to scientists, engineers,
teachers, students, and clinical providers. This book is suitable as both a professional reference
and as a text for a one-semester course for biomedical engineers or medical technology
students.
Youxin Mao
Institute for Microstructural Science,
National Research Council Canada
VII
Contents
1. Volumetric Image Registration of Multi-modality Images of CT, MRI and PET
2. Full Range Swept-Source Optical Coherence Tomography with Ultra Small
Fiber Probes for Biomedical Imaging
Youxin Mao, Costel Flueraru and Shoude Chang
3. Brain Imaging and Machine Learning for Brain-Computer Interface
Maha Khachab, Chafic Mokbel, Salim Kaakour, Nicolas Saliba and Gérard Chollet
4. Texture Analysis Methods for Medical Image Characterisation
VIII
Volumetric Image Registration of Multi-modality Images of CT, MRI and PET
1
Volumetric Image Registration of Multi-modality Images of CT, MRI and
1
PET
X
Guang Li and Robert W. Miller
Volumetric Image Registration of
Multi-modality Images of CT, MRI and PET
Guang Li and Robert W. Miller
National Cancer Institute, National Institutes of Health
Bethesda, Maryland,USA
1. Introduction
1.1 Biomedical Imaging of Multimodality
Three-dimensional (3D) biomedical imaging starts from computed tomography (CT) in
1960’s-1970’s (Cormack, 1963, Hounsfield, 1973) followed by magnetic resonance imaging
(MRI) in 1970’s (Lauterbur, 1973, Garroway et al, 1974, Mansfield & Maudsley, 1977). These
anatomical imaging techniques are based on physical features of a patient’s anatomy, such
as linear attenuation coefficient or electromagnetic interaction and relaxation. 3D biological
imaging (molecular imaging or functional imaging), such as positron emission tomography
(PET) and single photon emission computed tomography (SPECT), was also developed in
mid 1970’s (Ter-Pogossian, et al, 1975, Phelps, et al, 1975). They detect biological features
using a molecular probe, labelled with either a positron emitter or a gamma emitter, to
target a molecular, cellular or physiological event, process or product. So, the x-ray/γ-ray
intensity from a particular anatomical site is directly related to the concentration of the
radio-labelled molecular marker. Therefore, a biological event will be imaged in 3D space.
Since the concept of hybrid PET/CT scanner was introduced (Beyer, et al, 2000), the co-
registration of biological image with anatomical image offers both biological and anatomical
information in space, assuming that there is no patient’s motion between and during the
two image acquisitions. Other combined scanners, such as SPECT/CT and PET/MRI, have
also been developed (Cho, et al, 2007, Bybel, et al, 2008, Chowdhury & Scarsbrook, 2008).
Registration of biological and anatomical images at acquisition or post acquisition provides
multi-dimensional information on patient’s disease stage (Ling, et al, 2000), facilitating
lesion identification for diagnosis and target delineation for treatment.
In radiological clinic, although a particular imaging modality may be preferable to diagnose
a particular disease, multimodality imaging has been increasingly employed for early
diagnosing malignant lesion (Osman, et al, 2003), coronary artery diseases (Elhendy, et al
2002), and other diseases. Use of biological imaging enhances the success rate of correct
diagnosis, which is necessary for early, effective treatment and ultimate cure.
In radiation therapy clinic, multi-modality imaging is increasingly employed to assist target
delineation and localization, aiming to have a better local control of cancer (Nestle, et al,
2
Biomedical Imaging
2009). Radiation therapy (RT) contains three basic components: treatment simulation,
mm and time requirement of 15-20 minutes is sufficiently accurate and fast to meet the
treatment planning and treatment delivery (Song & Li, 2008). Simulation is to imaging a
clinical challenges of increasing utilization of multi-modality images in planning, increasing
patient at treatment condition for planning, based on which the treatment is delivered. In
adoption of image-guided delivery, and increasing throughput of patient treatments.
image-based planning, multimodality images, including CT, MRI and PET, can be registered
and used to define the target volume and location within the anatomy (Schad et al, 1987,
Chen & Pelizzari, 1989). In image-guided delivery, on-site imaging which provides patient’s
positioning image, is used to register to the planning CT image for accurate patient setup, so
that the target is treated as planned (Jaffray, et al, 2007).
Therefore, in both diagnostic and therapeutic imaging, image registration is critical for a
successful clinical application. Beyond the 3D space, 4D (3D+time) biomedical imaging has
become an emerging clinical research field, and some procedures have been adopted in the
clinic, such as 4DCT (Li et al, 2008a). Motion is inevitably present during imaging as well as
therapeutic processes, including respiratory, cardiac, digestive and muscular motions,
causing image blurring and target relocation. 4D medical imaging aims to minimize the
motion artefact and 4DRT aims to track and compensate for the target motion. Facing the
challenge of patient’s motion and change along the time, deformable image registration has
been intensively studied (Hill, et al, 2001, Pluim et al, 2003, Li et al, 2008b). Although it
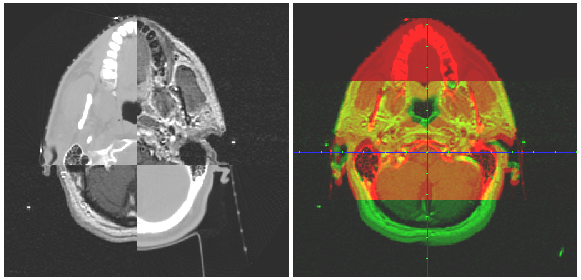
Fig. 1. Illustration of two common means of image alignment based on 2D planar views
remains as challenging topic, it will be only discussed briefly where it is needed, as it is not
(Only one of the axial slices is shown, and the sagittal and coronal series are not shown).
the main focus of this chapter.
The 3D visual representation or volumetric visualization (Udupa, 1999, Schroeder, et al,
2004) has recently been applied to evaluate the volumetric alignment of two or more 3D
1.2 Manual Image Registration
images (Xie, et al, 2004, Li, et al, 2005, 2007, 2008b and 2008c). This 3D volumetric image
Manual or interactive image registration is guided by visual indication of image alignment.
registration (3DVIR) technique aims to solve most of the problems associated with the
The conventional visual representation of an 3D images is 2D-based, three orthogonal
conventional 2D fusion technique by providing a fundamentally different, volumetric visual
planar views of cross-section of the volumetric image (West, et al, 1997, Fitzpatrick, et al,
representation of multimodality images. This volumetric technique has been successfully
1998). Here the discussion will be focused on anatomy-based image registration, rather than
designed, developed and validated, while it is still relatively new to the medical field and
fiducial-based (such as superficial or implanted markers) or coordinate-based (such as
has not been widely adopted as an alternative (superior) to the conventional 2D visual
combined PET/CT system). All clinical treatment planning systems utilize this visual
fusion technique. Two of the major obstacles for the limited clinical applications are that (1)
representation for checking and adjusting the alignment of two images. In details, there are
from 2D to 3D visualization, the clinical practitioners have to be retrained to adapt
several means to achieve the visual alignment verification: (1) the chess-box display of two
themselves to this new technique, and (2) this technique has not yet been commercially
images in alternate boxes; (2) the simultaneous display of two mono-coloured images; and
available to the clinic.
(3) the superimposed display of the two images with an adjustable weighting factor. Fig. 1
illustrates the first two of the three basic visualization methods.
1.3 Automatic Image Registration
The 2D visual-based fusion technique has been developed, validated and adopted for
Automatic image registration can improve the efficiency and accuracy of the visual-based
biomedical research as well as clinical practice (Hibbard, et al, 1987, Chen, et al, 1987,
manual fusion technique. There are three major components in any automatic image
Hibbard & Hawkins, 1988, Pelizzari, et al, 1989, Toga & Banerjee, 1993, Maintz & Viergever,
registration, including (1) registration criterion; (2) transformation and interpolation; and (3)
1998, Hill, et al, 2001). Throughout the past three decades, this technique has evolved and
optimization. These three components are independent of one another, so that they can be
become a well developed tool to align 3D images in the clinic. Multi-modality image
freely recombined for an optimal outcome in a particular clinical application. Here again,
registration is required (Schad et al, 1987, Pelizzari, et al, 1989) as more medical imaging is
the discussion will focus on anatomy-based rigid image registration, rather than fiducial-
available to the clinic. However, reports have shown that this well established technique
based or coordinate-based registration.
may suffer from (1) large intra- and inter-observer variability; (2) the dependency of user’s
cognitive ability; (3) limited precision by the resolution of imaging and image display; and
Before mutual information criterion (negative cost function) was developed in 1995 (Viola &
(4) time consuming in verifying and adjusting alignment in three series of planar views in
Wells, 1995), other algorithms were utilized, such as Chamfer surface matching criterion
three orthogonal directions (Fitzpatrick, et al, 1998, Vaarkamp, 2001). These findings have
(Borgefors, 1988, van Herk & Kooy, 1994) or voxel intensity similarity criterion (Venot, et al,
become a concern whether this 2D visual-based fusion technique with an accuracy of 1-3
1984). Mutual information is fundamentally derived from information theory and has been
Volumetric
Image Registration of Multi-modality Images of CT, MRI and PET
3
2009). Radiation therapy (RT) contains three basic components: treatment simulation,
mm and time requirement of 15-20 minutes is sufficiently accurate and fast to meet the
treatment planning and treatment delivery (Song & Li, 2008). Simulation is to imaging a
clinical challenges of increasing utilization of multi-modality images in planning, increasing
patient at treatment condition for planning, based on which the treatment is delivered. In
adoption of image-guided delivery, and increasing throughput of patient treatments.
image-based planning, multimodality images, including CT, MRI and PET, can be registered
and used to define the target volume and location within the anatomy (Schad et al, 1987,
Chen & Pelizzari, 1989). In image-guided delivery, on-site imaging which provides patient’s
positioning image, is used to register to the planning CT image for accurate patient setup, so
that the target is treated as planned (Jaffray, et al, 2007).
Therefore, in both diagnostic and therapeutic imaging, image registration is critical for a
successful clinical application. Beyond the 3D space, 4D (3D+time) biomedical imaging has
become an emerging clinical research field, and some procedures have been adopted in the
clinic, such as 4DCT (Li et al, 2008a). Motion is inevitably present during imaging as well as
therapeutic processes, including respiratory, cardiac, digestive and muscular motions,
causing image blurring and target relocation. 4D medical imaging aims to minimize the
motion artefact and 4DRT aims to track and compensate for the target motion. Facing the
challenge of patient’s motion and change along the time, deformable image registration has
been intensively studied (Hill, et al, 2001, Pluim et al, 2003, Li et al, 2008b). Although it
Fig. 1. Illustration of two common means of image alignment based on 2D planar views
remains as challenging topic, it will be only discussed briefly where it is needed, as it is not
(Only one of the axial slices is shown, and the sagittal and coronal series are not shown).
the main focus of this chapter.
The 3D visual representation or volumetric visualization (Udupa, 1999, Schroeder, et al,
2004) has recently been applied to evaluate the volumetric alignment of two or more 3D
1.2 Manual Image Registration
images (Xie, et al, 2004, Li, et al, 2005, 2007, 2008b and 2008c). This 3D volumetric image
Manual or interactive image registration is guided by visual indication of image alignment.
registration (3DVIR) technique aims to solve most of the problems associated with the
The conventional visual representation of an 3D images is 2D-based, three orthogonal
conventional 2D fusion technique by providing a fundamentally different, volumetric visual
planar views of cross-section of the volumetric image (West, et al, 1997, Fitzpatrick, et al,
representation of multimodality images. This volumetric technique has been successfully
1998). Here the discussion will be focused on anatomy-based image registration, rather than
designed, developed and validated, while it is still relatively new to the medical field and
fiducial-based (such as superficial or implanted markers) or coordinate-based (such as
has not been widely adopted as an alternative (superior) to the conventional 2D visual
combined PET/CT system). All clinical treatment planning systems utilize this visual
fusion technique. Two of the major obstacles for the limited clinical applications are that (1)
representation for checking and adjusting the alignment of two images. In details, there are
from 2D to 3D visualization, the clinical practitioners have to be retrained to adapt
several means to achieve the visual alignment verification: (1) the chess-box display of two
themselves to this new technique, and (2) this technique has not yet been commercially
images in alternate boxes; (2) the simultaneous display of two mono-coloured images; and
available to the clinic.
(3) the superimposed display of the two images with an adjustable weighting factor. Fig. 1
illustrates the first two of the three basic visualization methods.
1.3 Automatic Image Registration
The 2D visual-based fusion technique has been developed, validated and adopted for
Automatic image registration can improve the efficiency and accuracy of the visual-based
biomedical research as well as clinical practice (Hibbard, et al, 1987, Chen, et al, 1987,
manual fusion technique. There are three major components in any automatic image
Hibbard & Hawkins, 1988, Pelizzari, et al, 1989, Toga & Banerjee, 1993, Maintz & Viergever,
registration, including (1) registration criterion; (2) transformation and interpolation; and (3)
1998, Hill, et al, 2001). Throughout the past three decades, this technique has evolved and
optimization. These three components are independent of one another, so that they can be
become a well developed tool to align 3D images in the clinic. Multi-modality image
freely recombined for an optimal outcome in a particular clinical application. Here again,
registration is required (Schad et al, 1987, Pelizzari, et al, 1989) as more medical imaging is
the discussion will focus on anatomy-based rigid image registration, rather than fiducial-
available to the clinic. However, reports have shown that this well established technique
based or coordinate-based registration.
may suffer from (1) large intra- and inter-observer variability; (2) the dependency of user’s
cognitive ability; (3) limited precision by the resolution of imaging and image display; and
Before mutual information criterion (negative cost function) was developed in 1995 (Viola &
(4) time consuming in verifying and adjusting alignment in three series of planar views in
Wells, 1995), other algorithms were utilized, such as Chamfer surface matching criterion
three orthogonal directions (Fitzpatrick, et al, 1998, Vaarkamp, 2001). These findings have
(Borgefors, 1988, van Herk & Kooy, 1994) or voxel intensity similarity criterion (Venot, et al,
become a concern whether this 2D visual-based fusion technique with an accuracy of 1-3
1984). Mutual information is fundamentally derived from information theory and has been
4
Biomedical Imaging
extensively discussed in the literature (Hill, et al, 2001, Pluim, et al, 2003). It is worthwhile to
difficulty or with high accuracy requirement. We have found that pairing automatic MMI
mention that among existing criteria the common features in two different modality images
registration and the 3DVIR serves the best in terms of registration speed and outcome.
are best described by the mutual information, which can serve as the registration cost
The advantage of hybridized image registration is that it will take the advantage of multiple
function for maximization to achieve multi-modality image registration.
image processing techniques. Image segmentation/classification can extract more reliable
features from the original image to enhance image registration with the more informative
The transformation and interpolation are mathematical operations of the images. For rigid
features. Image (volumetric) visualization can enhance image registration, if a classified
image registration, only six degrees of freedom (three rotational and three translational) are
reliable anatomy is visualized and utilized as the registration landmark. Therefore, hybrid
in the transformation and the transformed voxels are assigned through interpolation (linear,
image registration remains a focus of clinical research (Li, et al, 2008b). Although feature
nearest neighbour, or Spline). For deformable image registration, however, the number of
extraction is often application specific and few algorithms can be employed across the
degree of freedom is dramatically increased, since all voxels are allowed to move (deform)
spectrum of all imaging modalities, hybrid image registration, such as the 3DVIR, has
independently and therefore the number of variables would be up to three times of the total
shown its promise to resolve particular clinical problems that require high accuracy.
number of voxels in an image. As a consequence, the performance of deformable image
registration becomes one of the bottlenecks, despite that several simplified algorithms have
been studied to address this challenging problem (Pluim et al, 2003, Li et al, 2008a & 2008b).
1.5 Visual Verification of Registration
Although automatic rigid image r