Here is the information you need to be able to ask the fundamentally important questions about health care in America. There is no doubt that this issue is still a major topic for our society and everyone should be equipped to be able to ask difficult and illuminating questions. Why is it so expensive, why are outcomes poor when compared to other Western nations, why is the public so angry, why if we already spend so much do we have to spend more to provide universal coverage when other countries do so at far less cost? Is there a way to cover all Americans and yet decrease not increase Federal and State spending?
What has happened to the healing patient-doctor relationship, why is American medicine so drug, device and test intensive?
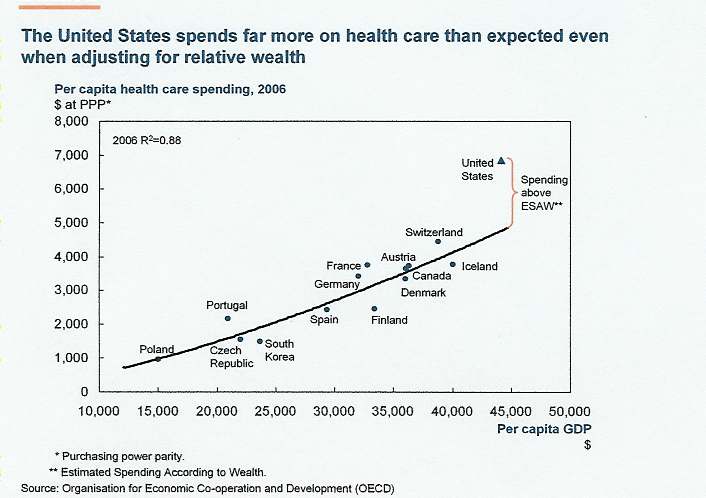
Healthcare today consumes about 17% of gross domestic product (GDP), approximately $7,600/person, almost twice as much as any other country, and is a major contributor causing manufacturing to leave this country along with good paying jobs. States, partly because of Medicaid spending, are not adequately funding public education; thus many youngsters are not prepared to participate in a world-wide competitive economy which then leads to increased poverty.
Despite spending this large fraction of our GDP on health care, we have approximately forty-five million uninsured individuals. The present attempts to provide universal coverage is calculated to consume 20-22% of GDP, which will worsen our manufacturing competitiveness and utilize taxes that could be spent on decreasing our deficit.
The good news is that by two completely different methods it has been shown that about one third ($700-800 billion) of our health care spending is of no benefit. The object of a thoughtful plan should be to understand the reasons why this very expensive non-beneficial care is taking place and how to address and rectify these factors. Not only would care improve, but there would be enough savings to provide universal coverage while spending less.
Unfortunately the recently passed Patient Protection and Affordable Care Act although providing for almost universal coverage does so by proposed large decreases in Medicare funding causing many or perhaps most hospitals to face financial ruin. The Act relies heavily on significant increases in Medicaid spending that will eventually put a greater burden on state budgets, decreasing their ability to fund public education, just the opposite of what is in our society’s best interest.
4
This law is primarily an insurance bill and does not examine the various forces acting on the patient-doctor relationship that have led to where we are today.
This electronic book will provide the information you need to better understand these forces and give you solutions that would allow us to have universal coverage at a lower not greater cost. You would then be better able to address this issue when questioning policy makers and “experts”. Future essays along with questions or comments about this material may be posted on my blog, http://drkennethfisher.blogspot.com ; I will do my best to address them in a timely manner.
5
Section 1 – The Ten Questions
I initially wrote these ten questions and the answers for my blog, which I own and is original with me and from which they have been copied and pasted. I believe you will find the questions and answers helpful as you try to understand the vast complexities of our health care system.
6
Overview of the Ten Questions
I often yearn for the days when we had news people like Walter Cronkite, Peter Jennings, the tenacious reporters from the New York Times and others who could truly think and had a keen eye for the issues at hand. They did their homework and, when conducting interviews or participating in Capitol Hill news conferences, asked pertinent, meaningful questions even if it made the person being questioned squirm. They examined all sides of an issue – good, bad, and everything in between – to bring balanced reporting to important national debates – balance that is decidedly missing now.
Congress has enacted a health care plan that simply won't work and will cost taxpayers a small fortune for generations to come. And, so far, no one in the media - either broadcast or print - has asked any of the questions that really need to be answered and addressed in order to bring reform that will work and won't break the bank.
Here are the questions I feel needed to be asked by the national media, and should have been asked as this process was getting underway. Possible answers will follow each question on succeeding pages.
1. What is medical consumerism and what factors do you believe exacerbate this issue? Are you familiar with Professor George Annas’s article on the Baby K case in the May 26, 1994 pages 1542-1545 issue of the New England Journal of Medicine regarding the impact it is having on medical care in this country? How do you think we should address this problem?
2. Various experts using different methods have determined that Americans presently spend about $700 billion a year on inappropriate non-beneficial care and that this excess spending is primarily due to physician practices.
What do you believe are the factors causing physicians to practice this way and how would you address these issues?
7
3. The business round table has stated that our present high health care costs as reflected by the percentage of gross domestic product (17%), that is much higher than other countries, is driving manufacturing and its high paying jobs out of this country. How should we address this issue?
4. Why does the cost of care in teaching hospitals vary so dramatically from hospital to hospital, as documented by the Dartmouth Atlas of Health Care, despite the fact that their physicians are salaried and do not charge fee for service?
5. Why do we have so many sub-specialists and so few primary care doctors despite the fact that primary care doctors are the key to providing coordinated care of high quality for less cost? How can we can we remedy this imbalance in the near future?
6. What has been the history of decreases in Medicare payments? Have they been successful and what effect do you believe these policies have had on American medicine?
7. What is the effect on working Americans of private insurance having to subsidize Medicare and Medicaid?
8. What do you think is the effect on state budgets of having to assume about 50% of the costs of Medicaid?
9. When can a patient reasonably utilize choice in care and in what situations are choices reasonably limited and who should determine when those conditions are reached?
10. What do you think is the result of cobbling together various constituencies in trying to pass a health care reform bill?
8
Answer to Question # 1
What is medical consumerism and what factors do you believe exacerbate this issue? Are you familiar with Professor George Annas’s article on the Baby K case in the May 26, 1994 (pages 1542-1545) issue of the New England Journal of Medicine regarding the impact it is having on medical care in this country? How do you think we should address this problem?
A) The concept of patient autonomy is problematical as its limits have not been defined.
B) Many Americans believe that a few hours at a web site is sufficient to adequately learn about a medical subject without understanding the complexities involved.
C) Drug and device advertising to the public promotes the newest most expensive drug/device as superior and your doctor is unaware of this marvelous advance. In reality direct advertising is an attempt by these companies to convince the public that their product is the newest and best when usually older and cheaper drugs/devices are just as effective1.
D) Hospitals and doctors have adopted a customer oriented business model to maximize revenue.
E) There are unresolved ambiguities caused by the Patient Self Determination Act (1990) which created the legal framework for advanced directives.2 Many ethicists and physicians have noted that advanced directives have the potential of turning the physician into a technician following instructions no matter how inappropriate.3 Questions arise about the limits of therapy in the absence of an advanced directive.
Although passed in 1990, these concerns are yet to be addressed by Congress.
F) Physicians practice defensive medicine because of the widespread fear of lawsuits. Our legal history is replete with cases that have demonstrated to 9
the physician community that logic and rationality are secondary to patients’/families’ requests and desires.
Two examples of this are the cases of Baby K and Helga Wanglie.
1) In the Baby K case an anencephalic baby (no cerebral cortex – no possibility for consciousness or human activity) was born by caesarian section in 1992. Although the physicians, hospital ethics committee, the court appointed guardian and the child’s father recognized the futility of further care, the child’s mother insisted on continuing care along with mechanical ventilation (breathing tube connected to a machine) if needed and pursued legal action. The trial court misinterpreted the Emergency Medical Treatment and Active Labor Act (EMTLA)4 by not considering the child as an integrated entity, but rather as a respiratory case. Professor Annas, Chair Department of Health Law, Bioethics & Human Rights at Boston University made several cogent statements about this case: 1) Knowing in advance that the fetus was anencephalic ,before delivery the physicians should have discussed with the mother that they would not use mechanical ventilation after birth. 2) The trial judge misinterpreted the intent of Congress in writing the law. 3) Congress mistakenly did not include wording such as, “within the bounds of good medical practice”. 4) We should be treating patients in light of what is best for them and not as objects to meet the needs of others.
5) To avoid medicine becoming a consumer product like toothpaste and in the process becoming unsustainably expensive, physicians will have to set standards for medical practice and follow them;5 to this date this has not happened
2) In the Helga Wanglie case, an 86 y/o women was in a persistent vegetative state for a year in an intensive care unit. The physicians concluded that in this case there was no chance of recovery and that hospice would be better for the patient. Her husband objected and sought relief from the courts, which found in favor of the husband; however, Helga died a few days after the verdict.6
What is needed to address medical consumerism and resolve the ambiguities between patient and doctor? I suggest:
10
1. Congress should amend the Patient Self Determination Act, The Americans with Disabilities Act and the EMTLA to contain the phrase, “within the bounds of good medical practice”. This would facilitate physicians developing and adhering to practice standards.
2. An advance directive should be completed at each hospital admission with guidance from physicians as to what is feasible in light of the patients overall condition, with seasoned physicians and a nurse available to adjudicate conflicts.
1Angell M. The Truth About the Drug Companies: How They Deceive Us and What to Do About It. Random House N.Y. N.Y. 2004 ISBN: 978-0-375-50846-2
2The Patient Self-Determination Act (PSDA) was passed by the U.S. Congress in 1990 as an amendment to the Omnibus Budget Reconciliation Act of 1990.
3Perkins HS. Controlling death: the false promise of advance directives. A n n a l s o f I n t e r n a l M e d i c i n e 2007; 147: 51-57 (PMID 17606961)
442 U.S.C. 1395 dd (1994) (amended 1997)
5Annas GJ. Asking the courts to settle standard of emergency care – the case of Baby K. e w E n g l a n d J o u r n a l o f N
M
e
d
i
c
i
n
e
1994; 330: 1542-1545 (PMID 8164726)
6Angell M. The case of Helga Wanglie; a new kind of “right to die” case. e w E n g l a n d J o u r n a l o f M e d i c i n e 1991; N
325: 511-512 (PMID 1852185)
11































Answer to Question # 2
Various experts using different methods have determined that we Americans presently spend about $700 billion on inappropriate non-beneficial care and that this excess spending is primarily due to physician practices. What do you believe are the factors causing physicians to practice this way and how would you address these issues?
A) There are multiple studies and estimates by experts leading to the conclusion that about $700 billion dollars per year are spent on unnecessary, inappropriate care in the United States.
Total Reimbursement Rates for Noncapitated Medicare per Enrollee, 2006, and Annual Growth in Medicare Reimbursements, 1992-2006, for the 25 Largest U.S. Hospital-Referral Regions Fisher E et al. N Engl J Med 2009;360:849-852
Peter Orzag (formerly head of the Congressional Budget Office, and Director of The Office of Management and Budget) using this data is quoted by Trapp D.,
“…estimated that up to $700 billion of the nation’s $2.3 trillion in annual health care spending does not improve outcomes”. 1
12
1) The Dartmouth Atlas of Health Care
Kenneth I. Shine , former President of the Institute of Medicine of The National Academies of Science in an editorial responded to an earlier version of this map saying, “….as much as 30% of health care costs might be eliminated without adversely affecting health care outcomes.”2
Arthur Garson and Carolyn L. Engelhard said in their book, “We do waste a lot of dollars on medical care, but this “one-half” estimate is based on an over-zealous interpretation of the data: the number is more likely one-third.”3 This one-third estimate exceeds $700 billion per year.
2) McKinsey & Co. December 2008 demonstrated by a different method that compared to other countries the U.S. wastes about $700 billion yearly on health care.
13
B) Dr. Arnold S. Relman former editor of the New England Journal of Medicine wrote, “Doctors, in consultation with their patients — not insurance companies, legislators, or government officials — make most of the decisions to use medical resources, thereby determining what the United States spends on medical care.”4
C) There are several factors causing physicians to practice in this way.
1. Doctors feel compelled to practice defensive medicine – the Massachusetts Medical Society has studied the cost of the yearly amount (2008) spent on defensive medicine in an attempt to minimize lawsuits. The study revealed that in Massachusetts a conservative estimate was $1.4 billion.5
2. Unrealistic demands by physicians placed on patients/families, in the name of patient autonomy, to make sophisticated and frequently non-beneficial and expensive medical decisions. These practices are well described by Dr. Atul Gawande in his book Complications.6
3. The present structure of advanced directives causes confusion and unrealistic expectations.7
4. Congress’s control of Medicare reimbursement rates under the influence of intense lobbying has resulted in the underfunding of primary care and overspending on technology and drugs.
5. Drug and device companies are now allowed to advertise to the public.
D) To address these problems I suggest the following actions: 1. Congress should amend The Patient Self Determination Act and related acts to contain the phrase, “within the bounds of good medical practice”.
2. Congress stipulates the use of a hospital admission form (below) for all Medicare patients. This form would enable patients to clarify their medical preferences with guidance as to medical feasibility along with an appeal mechanism in case of conflict.
3. The scope of peer review expanded to include consistent, uniform, organized oversight by senior physicians and nurses with knowledge 14
and experience in the practice of medicine and patient/family support to ensure that only beneficial care was being delivered.
4. Internal medicine sub-specialists should provide primary care for their patients who do not have a primary care physician.
1Trapp D. Obama budget sets stage for reform of Health care system, Medicare pay, American Medical News.
March 16, 2009 page 4
2Shine KI. Annals of Internal Medicine. 2003; 138:347-8. PMID: 12585834
3Garson A, Engelhard CL. Health Care Half Truths: Too many myths, not enough reality. N.Y., N.Y.
Rowman & Littlefield Publishers, 2007, Page 17
4Relman AS. Doctors as the key to health care reform. New England Journal of Medicine 2009:361: 1225-1227
PMID 19776404
5 www.massmed.org/defensivemedicine (accessed April 20, 2010) 6Gawande A. Complications: A surgeon’s notes on an imperfect science. N.Y., N.Y. Henry Holt & Company, 2002, Page 208
7Fisher KA, Rockwell LE, Scott M. In Defiance of Death: Exposing the Real Costs of End-of-Life Care. Westport, Connecticut , Praeger 2008, Page 11
15
New Hospital Admission Form
Appropriate Care Hospital Admission Form
Name __________________________ Med. Record #___________________
D.O.B. _________________________ Date __________________________
1. Is Patient capable of decision making: Yes ( ) No ( ) If No, who is responsible? Next of Kin/ guardian: ___________________
phone________________
2. Cardiopulmonary Resuscitation (CPR) is ordered on this patient: Yes ( ) No ( ) Place the following restrictions on CPR. DO NOT DO THE FOLLOWING: ( ) intubation ( ) chest compression ( ) resuscitation drugs ( ) cardioversion 3. When thought to be in an end of life situation by the medical team, I want to receive palliative care and consider placement in hospice: Yes ( ) No ( ) If No, the appropriate care I want is: ________________________________________
4. Other therapies this patient has chosen to refuse even though medically indicated are: 5. Other Stipulations or Concerns:
This form serves as a guide for physicians to carry out the wishes of the patient. There is a hospital physician team responsible for oversight of appropriate care, whose goal is to help define beneficial care appropriate for the patient (the benefit to the patient significantly exceeds the risks). An expanded peer review care committee is available for the patient should conflict arise.
Physician Signature __________________________
Patient Signature ___________________________
Witness Signature ___________________________
16
Answer to Question # 3
1. The business round table has stated that our present high health care costs as reflected by the percentage of gross domestic product (17%) that is much higher than other countries is pricing manufacturing and its high paying jobs out of this country. How should we address this issue?
2. During the recent health care debate one of the stated goals was that any health care bill should
increase the federal deficit. There was no
n
o
t
discussion on the effect that the percentage of gross domestic product (GDP) devoted to health care has on the overall economy and jobs. There was also no discussion on how a negative effect on the economy would decrease tax revenue and thus have a profound effect on the federal deficit. According to this line of reasoning two issues arise regarding the P
a
P
r
a
r
a
b
l
a
r
(1) will there be a significant
t
i
e
n
t
o
t
e
c
t
i
o
n
n
d
A
f
f
o
d
e
C
e
A
c
t
,
increase in the percentage of GDP devoted to health care and (2) if there is a significant increase of GDP devoted to health care would this cause a decrease in good paying American jobs?
Answer to (1) The Chief Actuary of the Centers for Medicare and Medicaid Services, Mr. Rick Foster, has calculated that when this law is in full effect it will increase the percentage of GDP devoted to health care to 21% and that the cost containment efforts will be largely ineffectual.
(http://republicans.waysandmeans.house.gov/UploadedFiles/OACT_Memorandu m_on_Financial_Impact_of_PPACA_as_Enacted.pdf).